|
howrahtb
|
|
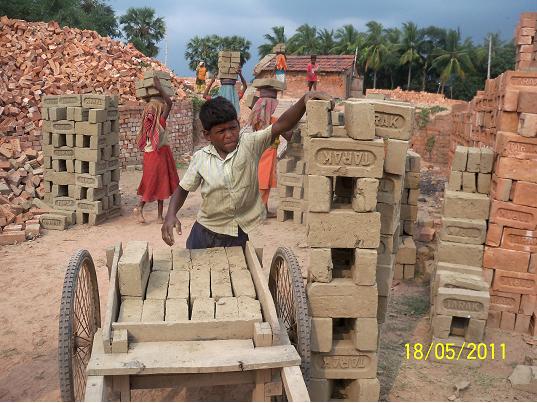
Maternal XN in brickfield Brickfields, large open area production sites for bricks along the river banks of the Ganges in southern West Bengal, are a “hot spot” of Vitamin A deficiency. In brickfields of southern West Bengal, a population of migrant worker families originating from Bihar, Jharkhand, Uttar Pradesh and Madhya Pradesh, does hard physical work on a pay per performance-basis to form, to dry and burn bricks from the mud and the sand of the river bank. These migrant worker families are called from their remote and underdeveloped villages in the above mentioned states of India and brought to the brickfields of West Bengal, where they stay and work for one season between the month of November and the month of July of the following year. In the rainy season, between August and October, brick production is not possible and the families return to their villages.
The migrant worker families are usually extraordinarily poor. All adults are illiterate and most of them are underweight or at the lower normal margin of the body mass index. The children of these families contribute to the physical work from the age of six onwards for minimal daily wages. There is no school education for the children of the brickfield families. No child of the brickfield migrant worker families has ever been vaccinated in their native places. The migrant worker families are not allowed to leave their production sites during the months of the working season and do therefore not mix with the local Bengalian population. An immunization team of our NGO attends brickfields every day during the season between November und July and tries to immunize as many children as possible. We avoid as well as even possible to disturb the production process on immunization days to keep good relation with the brickfield owners.
Parallel to the immunization work, we examined the extent of Vitamin A Deficiency among the mothers and children of the migrant worker families in the brickfields of southern West Bengal. We asked mothers who attended our free immunization camps for their children to take part in a structured interview about maternal night blindness in their recent pregnancy and about present day night blindness in their children of preschool age. Interviews were done during more than fifty immunization sessions in the years 2009 – 2011. Mothers attending immunization sessions with their children were interviewed about the appearance of night blindness in their most recent pregnancy within the last three years, which resulted in a live birth.1 Mothers with vision problems at daytime were excluded from the analysis. Mothers were asked furthermore about present day night blindness in their children of preschool age. This question referred to all their preschool age children, not only to those brought to the immunization camp on the day of the specific visit. As dates of birth of the children were usually not available,
all children were included in the analysis whose age was reported to be “one”, “two”, “three”, “four” or “five”, reflecting approximately the age group of 12 – 71 months. In this survey, children were not examined for Bitot`s spots. 944 consecutive mothers of brickfield migrant worker families attending immunization camps for their children were interviewed about the appearance of maternal night blindness during their most recent pregnancy, which resulted in a live birth within the last three years. 137 of the mothers (14.5%) reported having been night blind according to the above-mentioned criteria. In all cases, the night blindness resolved spontaneously after delivery.
This survey has some limitations. It reflects the extent of Vitamin A-deficiency in mothers and children of migrant worker families in the brickfields of southern West Bengal only and cannot be generalized to the overall population of parts of Bihar, Jharkhand, Uttar Pradesh and Madhya Pradesh, or to the native population of southern West Bengal.
Furthermore, this was not a door-to-door-survey in the colonies of the migrant worker families in the brickfield areas, but a survey among mothers attending immunization sessions for their children. Mothers attending immunization sessions or health camps for their children may have a different level of health consciousness in comparison with mothers not bringing their children, and this different level of health consciousness may also influence the level of Vitamin A-deficiency among them. Results may therefore not even be representative for the overall migrant worker family population in the brick fields of southern West Bengal. The here reported level of maternal night blindness among mothers from migrant worker families in brickfields of southern West Bengal belongs to the highest ever reported in the world. It raises questions about the nutritional status of the poor part of the population of Bihar, Jharkhand, Uttar Pradesh and Madhya Pradesh. Among the children of the migrant worker families on brickfields of southern West Bengal, there is a modest level of night blindness.
References: 1 – Christian, P. Recommendations for indicators: night blindness during pregnancy – a simple tool to assess Vitamin A Deficiency in a population. J Nutr 132: 2884S-2888S.
|



Copyright © 2010-2015 - www.howrahtb.com. All Rights Reserved
Site best viewed in IE 7 (1024*768) and above. If you have an older version of Internet Explorer, please upgrade your browser.